


Author: John Mattiacci | Owner Mattiacci Law
Published May 16, 2026
You may be reading this after a surgery that didn't make sense, a hospital stay that got worse instead of better, or a diagnosis that came too late. Often the first sign isn't a dramatic moment. It's a feeling that something was missed, something was delayed, or no one listened when the warning signs were there.
That feeling matters.
People usually call a lawyer after they've already asked themselves the same questions for days or weeks. Was this just a bad outcome? Was it a known risk? Or was it a preventable medical mistake? Those are hard questions, especially when you're trying to recover, manage bills, and make sense of confusing records. The law doesn't treat every poor result as malpractice, but it also doesn't excuse preventable harm just because it happened in a hospital.
When a Medical Outcome Feels Wrong
A common pattern looks like this. A patient goes in for what should be routine care. Then the timeline starts to break down. A nurse doesn't respond to a call light. A change in mental status isn't documented clearly. A test result sits too long without follow-up. A family member gets different answers from different people. By the time anyone says, “something went wrong,” the patient is already dealing with a much bigger injury.
That instinct to question what happened is often justified.
Medical errors are not always bizarre, isolated events. Many are recurring failures that hospitals, surgery centers, and care teams have struggled with for years. In The Joint Commission's Sentinel Event Data 2024 annual review summarized by NCBI Bookshelf, patient falls accounted for 49% of all reported sentinel events, followed by wrong-site, wrong-patient, or wrong-procedure surgery at 8% and delay in treatment at 8%. Those numbers matter because they show a pattern. The problem is often not one reckless person. It's a breakdown in supervision, communication, handoff, documentation, or basic safety steps.
What patients usually notice first
Most clients don't come in saying, “I experienced a breach of the standard of care.” They say things like:
- The story changed: One provider said everything was fine, then another admitted there had been a complication.
- The records don't match what happened: The chart may look neat, but the family remembers delays, confusion, or unanswered concerns.
- The recovery made no sense: Pain worsened, function dropped, or the patient needed emergency treatment after being told there was no serious issue.
A bad medical outcome can happen without negligence. But a preventable pattern, especially one tied to delay, poor communication, or the wrong procedure, deserves a close review.
When care feels wrong, the first goal is clarity. Naming the kind of error matters because different medical error types leave different evidence behind. A fall case looks different from a medication case. A delayed diagnosis case is built differently from a wrong-site surgery case. Once you know the category, you can start asking the right questions.
The Main Categories of Medical Errors
The phrase medical error types covers several different failures. Some happen during diagnosis. Others happen during treatment, monitoring, communication, or prevention. Patients often know the harm they suffered, but not the label that fits it. Putting the event into a category helps you figure out what records matter and what an attorney or medical expert will need to review.
A practical framework
The chart below gives a simple way to sort the most common categories.
| Error Category | Simple Definition | Example | What You Might Notice |
|---|---|---|---|
| Diagnostic error | A condition is missed, delayed, or identified incorrectly | Stroke symptoms treated as something minor | Symptoms worsen, treatment starts too late, test results weren't acted on |
| Treatment error | The right condition may be known, but care is carried out improperly | Wrong procedure or poor post-operative management | Unexpected complications, avoidable infection, sudden decline after treatment |
| Medication error | A drug is prescribed, dispensed, or given incorrectly | Wrong dose or a drug that conflicts with allergies | New symptoms after medication, oversedation, lack of expected effect |
| Communication error | Critical information isn't passed clearly between providers, staff, or the patient | Abnormal imaging result not relayed to the treating doctor | Conflicting instructions, missed follow-up, repeated retelling of the same history |
| Preventive error | Providers fail to take steps to avoid a foreseeable problem | Not addressing fall risk or not monitoring a known complication | A preventable injury happens during hospitalization or rehab |
| Documentation error | The chart is incomplete, inaccurate, or misleading | Medication administration or symptom changes recorded poorly | Records don't line up with what the patient or family experienced |
Why these categories matter legally
In malpractice work, the category shapes the investigation. A diagnostic case often turns on timing, symptom presentation, and what differential diagnosis should have been considered. A medication case may require looking at orders, pharmacy verification, MAR entries, barcode scanning, and the software used to enter the order. A communication case may rise or fall on handoff notes, nursing documentation, and whether anyone closed the loop on a critical result.
That's why basic documentation habits matter so much in healthcare. Even a training resource like CNA documentation practice questions and guidelines is useful for understanding how everyday charting, reporting, and patient communication are supposed to work. In a malpractice case, those ordinary records often become the backbone of proving what was said, what was observed, and what should have happened next.
A warning about labels
Patients sometimes focus on the most visible event and miss the underlying problem. A fall may not be just a fall. It may be the result of sedation, ignored alarms, poor staffing, or failure to respond to changes in condition. A bad surgical result may not be just a surgical issue. It may begin with a missed test result or an incomplete consent discussion.
So the right question usually isn't, “What went wrong in one moment?” It's, “What type of failure best explains the whole sequence?”
Mistakes of Action Versus Inaction
Some medical mistakes are obvious because someone did the wrong thing. Others are harder to see because no one did what should have been done. That distinction matters more than most patients realize.

Errors of commission
An error of commission is a wrong action. A provider gives the wrong medication. A surgeon operates on the wrong body part. A specimen is mislabeled. A patient with a known allergy receives the drug anyway.
These cases are often easier for families to recognize because there's an event they can point to. Something happened that plainly shouldn't have happened.
Errors of omission
An error of omission is a failure to act. A doctor doesn't order a test that the symptoms called for. A nurse doesn't escalate alarming vital signs. A critical radiology result isn't followed up. A patient isn't stabilized before transfer. No one responds in time.
These cases are frequently more dangerous from a legal standpoint because they hide inside silence, delay, and incomplete records. The patient may only see the final injury, not the missed opportunities that led there.
Practical rule: If your concern is “they did the wrong thing,” think commission. If your concern is “they never did what the situation required,” think omission.
Why omission cases are often harder
The omission versus commission distinction isn't just academic. It affects how a case is proved. According to MedLink's discussion of medical errors, fear of consequences was the most reported barrier to reporting medical errors at 63%. That matters because omission errors are especially likely to be softened, underreported, or buried inside vague charting.
A chart may show that a provider was “aware” of a symptom without showing what action was taken. It may document a call to a physician without documenting what information was conveyed. It may note “continue to monitor” when the actual question is why no one intervened.
What evidence tends to reveal inaction
In omission cases, the strongest proof often comes from absence and timing, not a dramatic admission. Important clues include:
- Missing orders: No imaging, no consult, no repeat labs, no transfer, no fall precautions.
- Delayed responses: Symptoms documented at one time, meaningful treatment only much later.
- Incomplete handoffs: One shift notices a problem, the next shift doesn't appear to know about it.
- Contradictory records: The hospital chart says the patient was stable while other entries show escalating distress.
That's why a thorough malpractice review doesn't just ask what was done. It asks what wasn't done, who knew, when they knew it, and what a competent provider would have done differently.
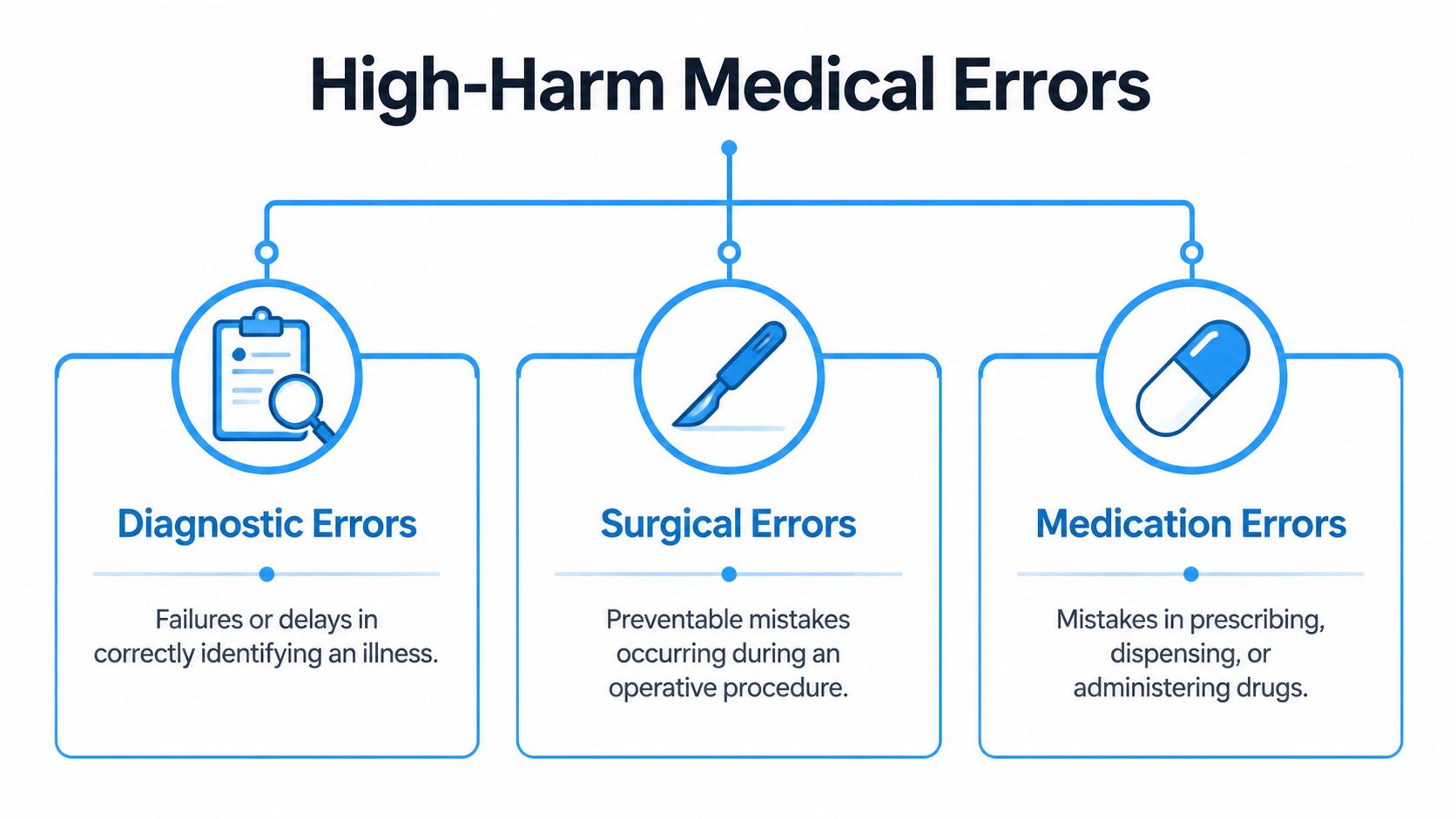
A Deeper Look at High-Harm Medical Errors
A patient goes to the emergency room with chest pain, gets discharged, and suffers a major cardiac event hours later. Another wakes up from surgery with a complication no one explained, or receives the wrong dose of a high-risk drug after a chain of entry and communication failures. These are the cases that often lead to the most severe harm, and they usually fall into three groups: diagnostic errors, surgical errors, and medication errors.
Diagnostic errors
Diagnostic cases are among the most damaging because the injury often comes from delay. The problem is not always that no one saw the patient. Often the patient was seen, evaluated, reassured, and sent home while the underlying condition kept getting worse.
A Johns Hopkins report on serious harms from diagnostic error estimated that about 795,000 Americans die or become permanently disabled each year because of diagnostic errors, and five conditions, stroke, sepsis, pneumonia, venous thromboembolism, and lung cancer, account for 38.7% of total serious harms. In practice, those numbers reflect what malpractice lawyers see repeatedly. A missed stroke window, a sepsis patient discharged too soon, or a suspicious lung finding left without follow-up can change the rest of a person's life.
These cases can involve an error of commission or omission. A doctor may actively diagnose the wrong condition and treat for that. Or the provider may fail to order imaging, fail to read a report correctly, fail to call the patient back, or fail to escalate obvious warning signs. For families trying to understand whether there is a case, the records matter more than the provider's later explanation. A useful starting point is understanding how medical negligence is proven in a malpractice claim, because diagnostic cases usually turn on timing, differential diagnosis, and whether a competent provider would have acted sooner.
Common warning signs include:
- Emergency-pattern symptoms that were not escalated
- Abnormal test results that were not communicated or acted on
- Repeat visits for the same worsening complaint
- Discharge instructions that did not match the risk in the chart
One sentence in a chart can matter. “Follow up with your primary doctor” may sound routine. In the wrong setting, it can reflect a dangerous failure to treat an emergency.
Surgical errors
Surgical cases are easier to spot, but they are still medicine-and-records cases, not outcome-only cases. A poor result after surgery does not automatically mean malpractice. Surgeons are allowed to face hard anatomy, unexpected bleeding, infection risk, and other known complications.
The legal question is narrower. Did the surgeon, anesthesiologist, nurse, or hospital depart from accepted practice in a way that caused harm?
Some surgical cases involve obvious breakdowns, such as wrong-site surgery, wrong-patient surgery, or retained instruments. Many others are less obvious. I often see claims tied to poor pre-operative planning, failure to obtain informed consent for a material risk, injury to surrounding structures, delayed recognition of internal bleeding, or failure to respond to post-operative deterioration.
The strongest evidence usually comes from the timeline. Operative reports, anesthesia records, sponge and instrument counts, recovery room notes, vital signs, post-op calls, consult requests, and follow-up imaging often show whether the complication was an unavoidable risk or a preventable mistake. That distinction matters in Pennsylvania and New Jersey, where the case must be supported by qualified expert review and tied to a clear departure from the standard of care.
Medication errors
Medication cases often involve more than one failure point. The mistake may begin with prescribing, continue during pharmacy verification, and reach the patient through bedside administration or a flawed electronic order entry system. That is one reason these cases require a wider review than patients expect.
As noted earlier in the article, analysts at ECRI found that health-IT-related medication error reports frequently involved wrong-dose events, usability problems, data-entry issues, and workflow support failures. Those findings matter because a medication injury is not always the fault of a single bedside provider. The order may have been entered incorrectly, displayed in a confusing way, or passed along without an adequate safety check.
High-risk medication cases often involve:
- Wrong dose, especially in pediatric, anticoagulant, insulin, or opioid cases
- Allergy alerts that were missed or overridden without justification
- Look-alike or sound-alike drugs
- Failure to monitor after giving a medication known to affect breathing, bleeding, or heart rhythm
- Medication reconciliation failures during admission, transfer, or discharge
These cases often combine action and inaction. Giving the wrong drug is an act. Failing to monitor the patient after that drug is given is an omission. Both can appear in the same chart.
What patients and families should watch for
Families usually recognize the warning signs before they know the legal terms. A diagnosis changes only after collapse. A patient declines after surgery and concerns are brushed aside. A new medication is followed by heavy sedation, breathing trouble, bleeding, confusion, or a rapid downhill course.
Those observations matter.
High-harm cases leave patterns in the records, and each category leaves a different one. Diagnostic cases often center on delayed recognition. Surgical cases often center on intraoperative decisions and post-op response. Medication cases often center on the chain from ordering to monitoring. A careful case review looks at each stage separately, then connects the evidence to the injury.
Proving Medical Negligence in Pennsylvania and New Jersey
Not every medical mistake becomes a winning malpractice claim. In Pennsylvania and New Jersey, the case has to be built around negligence, causation, and documented harm. The legal framework is straightforward. The proof is not.

The four parts of a malpractice case
Lawyers often break malpractice down into four basic elements.
| Element | What it means in plain English | Example |
|---|---|---|
| Duty | The provider owed the patient professional care | A doctor, nurse, hospital, or specialist was actually treating the patient |
| Breach | The provider fell below the accepted standard of care | A provider ignored symptoms that required testing or intervention |
| Causation | The breach caused harm, or made the outcome worse | Delay in diagnosis allowed a stroke, infection, or cancer to progress |
| Damages | The patient suffered real losses | Additional treatment, disability, lost income, pain, or death |
The defense usually fights hardest on breach and causation. They may argue the provider made a reasonable judgment call. Or they may say the underlying illness, not the medical mistake, caused the outcome.
Why some cases are harder than others
As StatPearls explains in its review of medical error subtypes, errors in surgery carry the highest risk of severe injury, while diagnostic errors are primarily cognitive and harder to prove. It also notes that malignancies, surgical complications, and neurological or cardiac problems are among the most frequently misdiagnosed conditions. That aligns with what malpractice lawyers see in practice. The more visible the mistake, the easier it is for a jury to understand. The more the case turns on thought process, judgment, and missed clues, the more expert testimony matters.
What Pennsylvania and New Jersey cases usually require
A serious malpractice claim in either state typically depends on several things happening early and correctly:
- Complete record collection: Hospital records alone aren't enough. Office records, imaging, pathology, EMS, rehab, and pharmacy materials may all matter.
- Expert review: A qualified expert has to explain what competent care required under the same circumstances.
- Procedural compliance: Malpractice cases have special filing requirements, including expert-related requirements such as a certificate or affidavit process depending on the jurisdiction and posture of the case.
- A damages narrative: The law values not just the mistake, but the human loss that followed it.
For a closer look at the legal proof involved, this guide on how to prove medical negligence walks through the core issues in a way most patients can use.
Strong malpractice cases don't just show that medicine is imperfect. They show that a specific provider or institution crossed a legal line and that the crossing changed the outcome.
What To Do If You Suspect a Medical Error
When people suspect malpractice, they often make one of two mistakes. They either wait too long because they don't want to “overreact,” or they confront the hospital before they've gathered the records. Neither helps.
Start with your health
Your first move is medical, not legal. Get appropriate follow-up care and, when needed, a second opinion from a provider who can evaluate the problem independently. If something serious is unfolding, don't delay treatment because you're trying to preserve a claim.
Protect the timeline
After that, start building a simple factual record while events are fresh.
Write down the sequence
Note symptoms, dates, names, medications, procedures, and what you were told. Include who was in the room when key conversations happened.Request your records
Ask for complete copies, not just discharge papers. That includes imaging, lab results, operative reports, nursing notes, medication records, and follow-up instructions.Save physical evidence
Keep prescription bottles, discharge packets, appointment summaries, photos of visible injuries, and any portal messages.
Be careful who you talk to
Hospitals and insurers may contact you before you understand what happened. Be polite, but careful. A risk manager is not your lawyer, and an insurance representative is not evaluating your case from your perspective.
- Don't guess about facts: If you don't know, say you don't know.
- Don't sign broad releases casually: They can give access to records beyond the issue in dispute.
- Don't assume an apology equals accountability: Many conversations sound supportive but don't explain the actual cause.
A lawyer can help you assess your options before you make statements that narrow them. This overview of how to sue a doctor for malpractice is a useful starting point if you're trying to understand the process in practical terms.
How a Malpractice Attorney Builds Your Case
A strong malpractice case starts with a reconstruction of the medical story. The chart matters, but it is rarely the whole story. I look for the timeline, the decision points, the missing follow-up, and the gap between what the records say and what the patient or family experienced.
That approach is especially important in omission cases. A delayed diagnosis, a missed test result, or a failure to respond to worsening symptoms often leaves fewer obvious fingerprints than a wrong-site procedure or a medication overdose. In those cases, the work is careful and methodical. The lawyer has to show what should have happened, when it should have happened, and how the delay or inaction changed the outcome.
Some cases also require a close review of system failures inside the hospital or practice. Medication injury, for example, may involve physician orders, pharmacy review, nursing administration records, barcode scanning, electronic alerts, and handoffs between departments. The final mistake may have been made by one person, but the proof sometimes shows a chain of preventable failures.
Expert review is usually the backbone of the case in Pennsylvania and New Jersey. The expert explains the applicable standard of care, identifies the departure from that standard, and addresses causation. That last part matters. It is not enough to show that care was poor. The evidence must connect the mistake, whether an act or a failure to act, to a specific injury that would probably have been avoided with proper treatment.
Damages require the same level of proof. A serious claim may include:
- Medical losses: additional hospitalization, corrective procedures, rehabilitation, medication, home care, and future treatment
- Income losses: missed work, reduced earning capacity, or the loss of a profession
- Human losses: pain, disability, loss of function, loss of independence, and the effect on daily family life
Good case building also means anticipating the defense. Hospitals often argue that the complication was a known risk, that the patient was already medically fragile, or that the outcome would have been the same even with proper care. That is why record review, qualified experts, and a clear timeline are so important. They turn a suspicion into proof.
If you want a practical overview of the legal process, this explanation of what happens in a medical malpractice case walks through the steps in plain English.
The strongest malpractice representation identifies the error, proves why it violated the standard of care, and shows how that violation caused real harm.